
Nyree Khachikyan *, Artur Manasyan, Stephanie Gaytan and Nafiseh Hashemi.
Hashemi Eye Care, 5353 Balboa Blvd#110, Encino, CA 91307.
*Corresponding authors: Nafiseh Hashemi, Hashemi Eye Care, 5353 Balboa Blvd#110, Encino, CA 91307.
Received Date: February 23, 2023
Accepted Date: February 28, 2023
Published Date: March 15, 2023
Citation: Khachikyan N, Manasyan A, Gaytan S, Hashemi N. (2023). “Hand Foot Mouth Disease Causing Fourth Nerve Palsy and Acute Maculopathy in Adult Male Patient: A Case Report and Review Literature”. Clinical Research and Clinical Case Reports, 4(1); DOI: http;//doi.org/03.2023/1.1063.
Copyright: © 2023 Nafiseh Hashemi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Hand, Foot, and Mouth Disease (HFMD) is a common viral infection that typically affects children, and rarely affects adults. We present a case of 31-year-old male without any significant prior medical history who presented with vertical diplopia and blurry vision after getting HFMD from his son. Upon examination, the patient was found to have right fourth nerve palsy and significant sub-macular edema in the left eye, an uncommon presentation of the disease. MRI of the brain and orbit, and bloodwork was normal except for a slightly elevated ESR level. The patient was started on an antiviral treatment of Valacyclovir for 21 days and a tapering treatment of oral steroid which significantly improved the macular swelling and double vision.
Purpose:
To report on the rare presentation of HFMD in an adult and increase knowledge of possible uncommon visual complications, such as fourth nerve palsy causing double vision and significant macular swelling.
Introduction :
Hand, Foot, and Mouth Disease is a viral infection that is caused by the coxsackie virus, a member of the enterovirus family [1]. It most typically affects children and presenting symptoms include a low-grade fever, rashes and sores on the hands, feet, and mouth as the name of the disease suggests. Diagnosis is usually made by inspection of the characteristic lesions on the hands and feet [2]. Recovery time ranges between 7-10 days and usually does not require any medical intervention, it resolves on its own [3]. The infection is rarely seen in adults. Currently, while there are a few cases of HFMD in adults with ocular presentations such as acute idiopathic macular edema, there are even fewer cases of HFMD reported that have resulted in nerve palsy, with double vision as a symptom of the patient.
Case Report:
The patient is a 31-year-old male who presented with red spots on his hands (Figure 1), headaches, blurry vision, and diplopia. He reported that his son, who attends daycare, was recently infected with Hand Foot and Mouth Disease. The patient’s visual acuity at the time of visit was 20/20 in both eyes with prescription glasses. Color vision was 11/11 in the right eye and 10/11 in the left eye. Intraocular pressure was 12mmHg in the right eye and 11mmHg in the left eye, which is within the normal range. Visual field exam to map the patient’s peripheral vision showed scattered scotoma in the left eye. On sensorimotor exam to measure the double vision, the patient was 3PD right hypertropia in primary gaze, increased in left gaze and right head tilt. These measurements indicated right fourth nerve palsy. On dilated eye exam and OCT of the macula, the patient was found to have sub-macular fluid in the left eye. (Figure 2). A Roth spot, a retinal hemorrhage characterized by a white center and indicative of systemic illness, was also found in the left eye. OCT of the optic nerve showed a normal RNFL thickness of 104 microns OD and 107 microns OS. An urgent MRI of the brain and orbit was ordered to rule out any compressive pathologies which may have caused the sudden onset of diplopia, and bloodwork was ordered to rule out other possible diseases prior to starting any treatment. MRI, and bloodwork was normal except for a mildly elevated ESR, indicative of the recent infection. The patient was started on a 21 day treatment of the antiviral medication Valacyclovir, taking 1 gram 3 times a day. Three days after starting the antiviral treatment, the patient also started a steroid prednisone treatment, beginning with 60 mg with tapering down by 10mg every three days.
The patient returned to the clinic after 2 weeks for a follow up. The diplopia had resolved in primary and right gaze, with residual 3RHT in left gaze. OCT of the macula showed no more sub-retinal fluid in the left eye (Figure 3). Fundus photo and dilated eye exam showed a macular scar in the left eye (Figure 4). The patient is currently being monitored and expected to make a full recovery.

Figure 1a-c: Patient’s hands covered in red spots following HFMD infection.
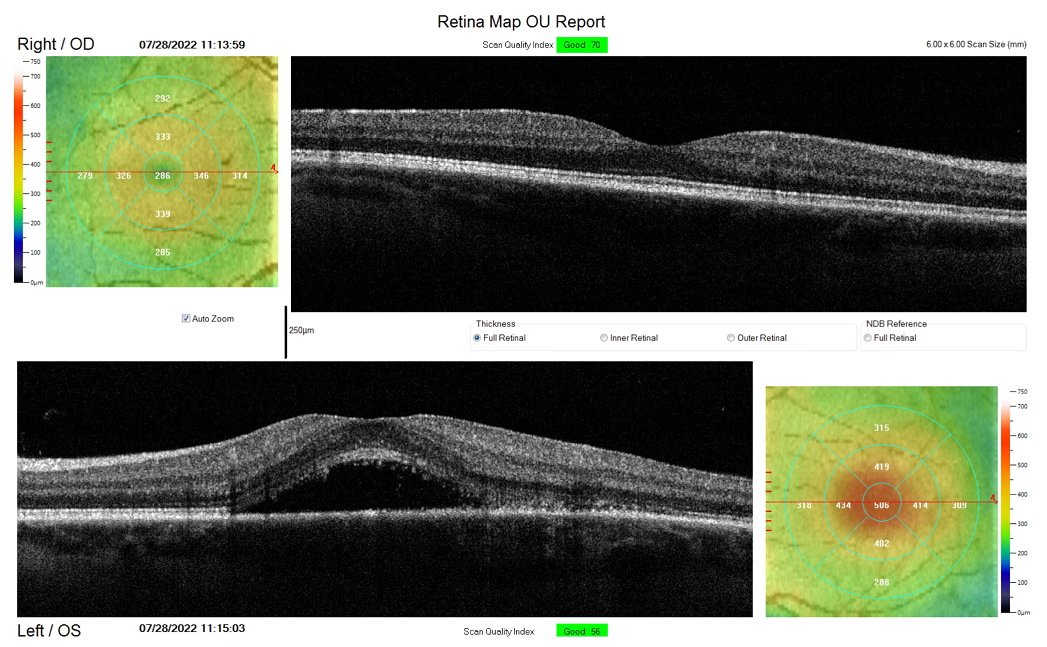
Figure 2: OCT Mac at initial visit showing fluid in left retina.
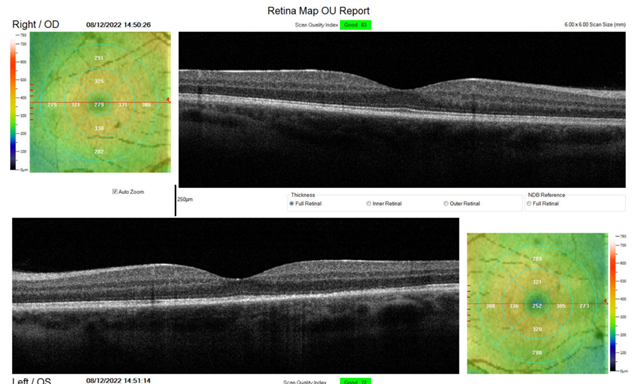
Figure 3: OCT Mac showing normal retinas in left and right eyes, and no more fluid in the left macula.
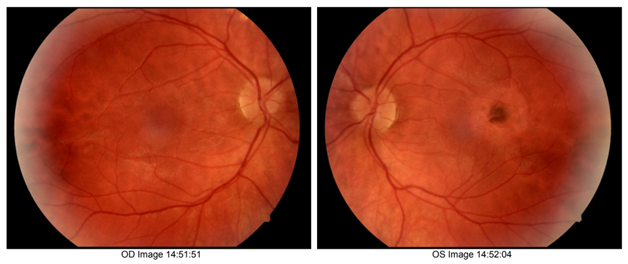
Figure 4: Fundus photo following treatment which shows macular scar in left eye.
Discussion:
Hand Foot Mouth Disease is a viral infection that most commonly affects young children under the age of 5 [4]. The most common symptoms include fever, sore throat, sores all over the hands, feet, and mouth (commonly referred to as herpangina), and an itchy skin rash. Although the majority of those infected with this disease are young children, adults can be infected with the coxsackie virus that causes HFMD as well; many don’t show symptoms, and those who do are often misdiagnosed with other diseases due to the rarity of the occurrence of HFMD in adults. There are currently very few reported cases of HFMD causing nerve palsy or acute idiopathic maculopathy in adults.
In one severe case of enterovirus infection causing HFMD in a 37-year old woman without any past serious illness, symptoms included diplopia, tremor, unsteadiness, and stiffness. The infection caused encephalitis; she fully recovered in 3 months after a treatment of acyclovir and cefotaxime [5]. Similarly, a 41-year old male was reported to have encephalitis following coxsackievirus infection, although this adult, unlike the former, was immuno-suppressed due to being on rituximab treatment. He also experienced double vision, as well as fever, headache, and gait unsteadiness [6]. Our presented patient, although having diplopia, did not experience any encephalopathic symptoms like unsteadiness or tremor.
In cases without diplopia or any observed nerve palsies, a 24-year old male presented with 20/200 vision in the left eye, and also had fever, sore throat, mouth ulcers, and sores in the palmoplantar and perioral region. OCT of the macula showed disruption of the ellipsoid layer and fundus exam showed subretinal exudate in the left eye [2]. The patient’s symptoms resolved and his vision corrected back to 20/20 after three months. In another case, a 36-year-old male who also had sores on his hands was examined by an ophthalmologist due to a small, abnormally bright area in his left visual field. Upon examination, the patient had a fundus lesion with pigment attenuation and aggregation present, which was not present two years prior at his regular eye check-up, so it is believed the HFMD caused this [7]. In another case of a 30-year-old man, outer retinitis was observed, including retinal hemorrhage and subretinal fluid. Eight weeks following the initial visit, visual acuity had improved from 20/50 to 20/25 in the affected eye and a slightly irregular IS/OS line was still present [8]. Two more cases reported involving a 30-year-old woman and a 38-year-old man showed evidence of a lesion in the retina found on the ophthalmologic exam [9]. Both patients’ symptoms resolved without intervention and only left a scar on the retina; visual acuity improved to 20/20. In one particular patient, while the characteristic lesions on his palms and feet resolved completely after some time, the visual symptoms that began as a result of HFMD persisted for five months, showing that timelines of the illness are variable and it can’t be certain whether all symptoms will resolve without any treatment [10]. While most reported cases were resolved without any intervention, one case of a 35-year old woman with macular intraretinal hemorrhage, pigmentary changes and thickening of the retina resolved after tapering of prednisone oral steroid [11]. Throughout these specific cases, diplopia in addition to visual field defects was not a reported symptom, and nerve palsy was not a diagnosis in addition to the maculopathy, as it was in our patient’s case.
Conclusion:
There have not been many reported cases of Hand Foot Mouth Disease in adults that have caused acute idiopathic maculopathy, and even fewer that have caused any nerve palsy. It is important to get a full history of patients prior to diagnosis, including any recent infections they or their family members have had. It is also important to be observant of other symptoms, as the sores commonly seen on the hands and feet of HFMD patients can be a defining factor in arriving at the correct diagnosis.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org